Emergency medical care for children. Major emergencies in children
▲ Diagnosis of major emergencies.
▲ Urgent help in emergency conditions.
ASTHMATIC STATUS
This is a long-term persistent obstruction respiratory tract, in which bronchodilators that previously relieved an asthma attack do not give an effect. Unlike an attack of bronchial asthma, including a protracted one, the leading role in the pathogenesis of status asthmaticus is played not by bronchospasm, but by edema, inflammation, dyskinesia of bronchioles, small bronchi filled with viscous, unexpelled sputum. The cessation of sputum drainage using natural mechanisms indicates the transition of a protracted attack of bronchial asthma to status asthmaticus. With obstruction of the respiratory tract by viscous sputum that is not coughed up, the addition of edema and inflammation of the bronchioles and small bronchi, inhalation becomes difficult, exhalation becomes active and elongated. In these cases, when inhaling, the bronchi expand, letting more air into the lungs than the patient can exhale through the narrowed and filled with viscous sputum bronchi. He tries to activate the exhalation, strains the pectoral muscles, which causes an increase in intrapleural pressure. At the same time, small bronchi are compressed, i.e., expiratory closure of the lower respiratory tract occurs, and then expiratory stenosis also joins - prolapse of the membranous part of the trachea and main bronchi into the lumen of the respiratory tract during inspiration. The respiratory muscles perform a huge, but inefficient work, expending a large number of oxygen. As a result, respiratory failure increases, hypoxia increases. Right ventricular failure gradually joins: the right ventricle has to overcome high intrathoracic pressure. Persistent obstruction of the respiratory tract with viscous sputum can be considered the first stage of status asthmaticus, right ventricular failure - the second, and metabolic disorders, expressed in hypoxia, respiratory and metabolic acidosis, hypohydration and adrenal insufficiency with all its consequences - the final. The most important component of respiratory failure in status asthmaticus is a violation of the drainage function of the respiratory tract, caused by hypersecretion and mainly a change in the consistency of sputum (it becomes viscous and is not removed by the natural mechanisms of cleaning the lungs).
clinical picture. There are three stages of an asthmatic condition. The first stage is similar to a prolonged attack of suffocation. At the same time, the patient develops refractoriness to sympathomimetics, develops violations of the drainage function of the bronchi (sputum does not go away), an asthma attack cannot be stopped for 12 hours or more. Despite the severity of the patient's condition, changes gas composition blood remains insignificant: moderate hypoxemia (P0l 70-80 mm Hg) and hypercapnia (PCo2 45-50 mm Hg) are possible, or, conversely, due to hyperventilation - hypocapnia (PCo2 less than 35 mm Hg). Art.) and respiratory alkalosis.
The asthmatic condition of the II stage is characterized by progressive violations of the drainage function of the bronchi, the lumen of which is filled with thick mucus. Gradually, the “silent lung” syndrome is formed: over certain areas of the lungs, the previously determined wheezing wheezes cease to be heard. There are sharp violations of the gas composition of the blood with arterial hypoxemia (PCo2 50-60 mm Hg) and hypercapnia (PCo, 60-80 mm Hg), mainly due to mixed acidosis. The patient's condition becomes extremely severe: consciousness is inhibited, the skin is cyanotic, covered with sticky sweat, marked tachycardia is noted, blood pressure tends to increase.
asthmatic condition III degree characterized by significant dysfunction of the central nervous system with the development of a picture of hypercapnic and hypoxemic coma on the basis of the sharpest violations of the gas composition of the blood (PCo, more than 90 mm Hg, P0l less than 40 mm Hg).
Treatment. Intensive therapy is indicated: A restoration of airway patency (improvement of the rheological properties of sputum, lavage of the bronchial tree and elimination of expiratory stenosis); A decrease in the harmful effects of hypoxia; And normalization of hemodynamics and correction of metabolism.
To liquefy sputum, aerosol inhalations of warm sterile water, isotonic sodium chloride solution, 0.5-1% sodium bicarbonate solution are prescribed. Facilitates the drainage of the respiratory tract intravenous infusion of crystalloid solutions. In addition, the goal of fluid therapy is to correct hypovolemia. Infusion therapy provides for the introduction during the first hour of ringerlactate (12 ml / kg), then 5% glucose solution and isotonic sodium chloride solution in a ratio of 1: 2 (100 ml / kg / day). To eliminate bronchospasm, high doses of aminophylline are administered through a perfusor (20-40 mg / kg / day at a rate of at least 2 ml / h). The effectiveness of the drug is evaluated by diuresis. Intravenous administration of glucocorticoids is indicated. They have a non-specific anti-inflammatory effect, inhibit the production of antibodies, promote the release of mediators from mast cells, restore the reaction of p-adrenergic receptors to catecholamines, and relax the muscles of the bronchi. Preference is given to dexazone (initial dose 0.3-0.4 mg/kg, then 0.3 mg/kg). The intensive care complex also includes heparin (100-300 IU / kg / day), antiplatelet agents. Oxygen therapy begins with the supply of warm humidified oxygen through a nasal catheter (oxygen concentration in the respiratory mixture 40%, gas flow 3-4 l/min). With an increase in Pco, and severe initial hypercapnia, mechanical ventilation is indicated.
HYPOGLYCEMIC COMA
Hypoglycemic coma- an acute condition that develops with a rapid decrease in the concentration of sugar in the arterial blood and a sharp drop in the utilization of glucose by the brain tissue.
Etiology. This condition occurs in cases of insufficient intake of glucose into the blood or increased excretion from the body, as well as in violation of the balance between these two processes. It is observed in patients with diabetes mellitus with an excess of injected insulin and inadequate intake of carbohydrate foods. A hypoglycemic symptom complex may develop in cases of using certain medicines(hypoglycemic sulfonamides), with a number of clinical syndromes accompanied by increased secretion of insulin (insulin-producing tumors). Unlike diabetic hypoglycemic coma develops suddenly, loss of consciousness occurs in a matter of minutes.
clinical picture. Characteristic features: profuse sweat, pallor and moisture of the skin, moisture of the tongue, superficial rhythmic breathing, no odor of acetone from the mouth and hypotension of the eyeballs. Jaw lockjaw, positive Babinski's symptom (on one or both sides) are possible. In addition, tachycardia, deafness of heart tones, arrhythmia, lability of blood pressure, a sharp decrease in blood sugar, the absence of sugar and acetone in the urine are noted.
Treatment should begin immediately: intravenously - concentrated glucose solutions (20%, 40%) without insulin (until the child shows signs of consciousness); inside - warm sweet tea, honey, jam, sweets, sweet semolina, White bread(with mandatory control of blood sugar).
DIABETIC COMA
Pathogenesis. Diabetic coma develops with the rapid progression of metabolic disorders as a result of late diagnosis of diabetes mellitus. The causes of coma in diabetic patients can be a gross error in the diet (eating a meal containing a large amount of sugar and fat), the cessation of the administration of insulin and other drugs that reduce blood sugar, as well as their inadequate doses. Exacerbation of diabetes is possible with mental and physical trauma, stressful situations, infections, diseases of the gastrointestinal tract, when the intake, absorption and passage of food are disturbed, which leads to starvation of the body. In cases of increasing insulin deficiency, there is a violation of the utilization of glucose by tissues, the processes of its oxidation and energy use cells, decreased permeability cell membranes for glucose. The synthesis of glycogen in the liver is disrupted, fatty degeneration develops. The breakdown of glycogen intensifies, compensatory formation of glucose from proteins and fat occurs. Hyperproduction of the insulin antagonist - glucagon and contrainsular hormones (STH, ACTH, catecholamines), which have a fat-mobilizing effect, contributes to an increase in blood glucose levels up to 28-40 mmol / l (500-700 mg%) or more. Hyperglycemia leads to an increase in the osmotic pressure in the extracellular fluid, resulting in intracellular dehydration. Insulin deficiency leads to a sharp limitation of the body's ability to use glucose to cover its energy costs and stimulates the compensatory breakdown of fats, to a lesser extent proteins. Violation of redox processes and intense protein breakdown in the liver lead to metabolic disorders, accompanied by the accumulation of ketone bodies, nitrogenous wastes and the development of uncompensated acidosis. Glucose, ketone bodies, nitrogenous slags begin to be excreted in the urine. The osmotic pressure in the lumen of the renal tubules increases, and renal reabsorption decreases, which causes polyuria with a large loss of electrolytes - potassium, sodium, phosphorus, chlorine. In connection with hypovolemia, which develops as a result of dehydration, severe hemodynamic disturbances occur (fall in blood pressure, decrease in stroke volume of the heart, decrease in glomerular filtration). Clinically, this is manifested by a collaptoid state and a decrease in urine output, up to anuria.
clinical picture. Coma develops gradually over several hours or days. There are fatigue, weakness, thirst, severe headaches, dizziness, ringing in the ears, agitation, insomnia, followed by lethargy, apathy and drowsiness, anorexia, nausea, vomiting, polyuria. Characterized by dryness of the skin and mucous membranes, dry tongue coated with a brown coating, the smell of acetone from the mouth, tachycardia, decreased blood pressure, muffled heart sounds, and sometimes arrhythmia. In diabetic coma, 4 stages of impaired consciousness are distinguished: I - stupor (the patient is inhibited, consciousness is somewhat confused); II - drowsiness, somnolence (the patient falls asleep easily, but can independently answer questions in monosyllables); III - stupor (the patient is in a state deep sleep and only comes out
Under the influence of strong stimuli); IV - actually coma (complete loss of consciousness, lack of response to stimuli).
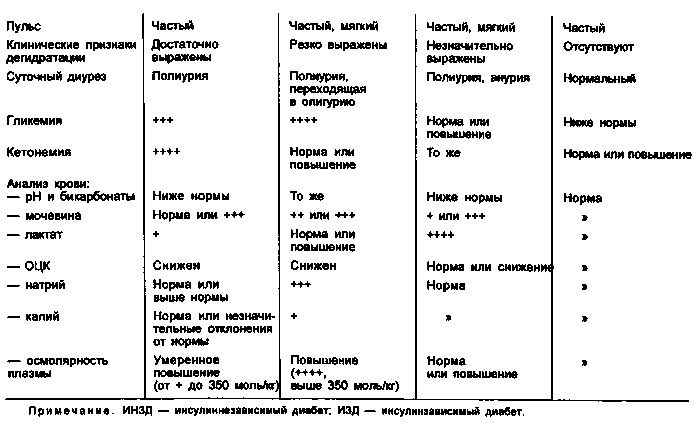
Diabetic coma should be differentiated from uremic and hepatic coma. In diabetic coma, hyperglycemia and glucosuria, the smell of acetone from the mouth, low blood pressure are pronounced; with uremic - the smell of urea, a high content of toxins in the blood, a sharp increase in blood pressure; with hepatic - a specific smell (of the liver) from the mouth, yellowness of the skin and mucous membranes, hemorrhages and scratching on the skin, enlargement and soreness of the liver, dyspepsia, bilirubinemia, urobilin - and bilirubinuria.
Differential diagnostic signs of coma, developing in patients with diabetes mellitus, see table. one.
The treatment is complex: the introduction of insulin, the fight against acidosis and dehydration. Insulin therapy should be strictly individual. If the child has not previously received insulin, then this drug is administered at a dose of 1 U / kg. The first dose of insulin for preschool children is 15-20 units, for schoolchildren 20-30 units. If the child has previously undergone insulin therapy, he is prescribed at the same time the same daily dose that he received before the onset of coma. At the same time, in order to avoid hypoglycemia, 5% glucose solution and isotonic sodium chloride solution are injected intravenously in a 1:1 ratio. Repeated injections of insulin are made in the first 6 hours at intervals of 1-2 hours (at the rate of 1 U / kg). As the general condition improves, the intervals between injections increase. The total dose of insulin used to bring a child out of a coma, as a rule, does not exceed 150 IU / day, but sometimes it is higher. In the first days after coma, insulin is administered 3-4 times a day under the control of blood and urine sugar, then they switch to a 2-time administration of the drug. Infusion therapy for the purpose of rehydration includes isotonic sodium chloride solution in the first days, Ringer's solution and 5% glucose solution in a ratio of 1:1 in the following days. The total volume of injected fluid is determined at the rate of 100-150 ml/kg/day. Subsequently, the amount of glucose in the injected fluid is increased, and potassium is added to it. At the same time, 1 unit of insulin should account for at least 1 g of dry glucose. When compiling an infusion therapy program, the total amount of fluid is calculated based on the needs of the body and pathological losses. Antibiotics are prescribed to prevent secondary infection. After removing the child from a coma, enteral nutrition is indicated (physiological diet with fat restriction).
RESPIRATORY INSUFFICIENCY
Etiology. The development of respiratory failure depends on many reasons, the main of which are violations of the central regulation of respiration, the muscular activity of the apparatus respiratory complex and airway patency. Respiratory failure causes a change in the ratio of pulmonary ventilation and gas perfusion, which is very pronounced in lung diseases: bronchial asthma, emphysema, bronchiolitis, pneumonia, tumors, malformations.
Violation of the central regulation of respiration occurs as a result of trauma, impaired cerebral circulation, edema and swelling of the brain of various etiologies, damage to the peripheral neuromuscular complex, both infectious and toxic.
Violation of the airway patency is observed with aspiration of amniotic fluid, stomach contents, obstruction of the airways by foreign bodies, swelling of the subglottic space of infectious, allergic and traumatic genesis, congenital diseases, malformations.
clinical picture. One of the early signs is shortness of breath, often with the participation of accessory muscles. Notice the color of the skin. More often they are cyanotic, but their gray pallor associated with microcirculation disorder and pronounced hypoxia is more dangerous. Characterized by tachycardia or tachyarrhythmia, in more severe cases, bradycardia. Due to respiratory failure, visceral functions are disturbed (diuresis decrease, sometimes intestinal paresis, acute erosions and ulcers in the digestive tract).
Treatment of respiratory failure: A prompt restoration of airway patency (if there is no injury cervical spine and neck, it is necessary to tilt the child’s head back as much as possible and put a roller under his shoulders; to prevent retraction of the tongue, introduce oral or nasal air ducts); And at the same time, you need to actively suck out the contents from the upper respiratory tract, trachea under the control of a laryngoscope; And the most effective method restoration of airway patency is bronchoscopy, nasotracheal intubation allows you to maintain bronchial patency for a long time; And to improve the rheological properties of sputum and enhance the drainage function of the bronchial tree, aerosol inhalations of mucolytics and isotonic sodium chloride solution are used (it is better to use a sound inhaler as a spray); And oxygen therapy during spontaneous breathing is used under the control of P0i and fractional oxygen concentration in the respiratory
Noy mixture (optimal oxygen concentration 40%). The oxygen concentration in the gas mixture depends on the gas exchange function of the lungs and can fluctuate over a wide range even in the same patient during the day; And artificial lung ventilation (ALV) helps to eliminate hypercapnia, hypoxia, catecholemia, improve ventilation perfusion ratios, normalize pH, restore metabolic processes and microcirculation. IVL is carried out in the conditions of the intensive care unit.
CIRCULATION DISORDERS
The cause of circulatory disorders can be heart or vascular insufficiency, often a combination of both.
Vascular insufficiency Occurs when the ratio between the volume of circulating blood (CBV) and the capacity of the vascular bed changes. The main factors in the development of vascular insufficiency are a decrease in BCC and a violation of vasomotor innervation.
clinical picture. Symptoms of acute vascular insufficiency: pallor of the skin, cold sweat, narrowing of peripheral veins, a sharp decrease in blood pressure, frequent and shallow breathing. Vascular insufficiency manifests itself in the form of fainting, collapse and shock.
Goals of intensive care: A restoration of BCC; And improvement of microcirculation; And the elimination of acidosis and metabolic disorders; And in acute vascular insufficiency, the use of painkillers, antihistamines and sedatives, oxygen therapy are indicated.
Acute heart failure in children(more often left ventricular) develops as a result of bacterial and toxic damage to the myocardium in viral and bacterial infections, poisoning, rheumatic diseases, heart defects, acute renal failure and other endotoxicoses. Right ventricular failure occurs, as a rule, with long-term chronic processes in the lungs ( bronchial asthma, chronic pneumonia, pulmonary and heart defects, emphysema, spontaneous pneumothorax).
clinical picture. The main symptoms: cyanosis of the skin, shortness of breath, expansion of the boundaries of the heart, tachycardia, deafness of heart tones, pastosity of tissues, liver enlargement, dyspeptic disorders.
Goals of intensive care: A reduction of hypoxia and hypoxemia; And unloading small and great circle blood circulation; And improvement of the contractile function of the myocardium; A correction of electrolyte and metabolic disorders.
Inhalation of oxygen contributes to an increase in its supply to the tissues, a decrease in shortness of breath, tension in the respiratory muscles and vasoconstriction in the lungs. To reduce blood flow to the heart, diuretics (lasix, furosemide) are used, for arterial hypertension - ganglion blockers (5% pentamin solution), broncho- and antispasmodics (2.4% solution of eufillin, papaverine, antianginal drugs and peripheral vasodilators (1 % solution of nitroglycerin, 0.1% solution of perlinganite or isoket, naniprus), angiotensin-converting enzyme inhibitors (kapoten and its derivatives), calcium antagonists (nifedipine), drugs with a positive inotropic effect (dopamine, dobutrex, dobutamine).To improve myocardial contractility cardiac glycosides are used.Correction of metabolic disorders is carried out by introducing 5% and 10% solutions of glucose, potassium and calcium salts, vitamins of group B, vitamin C. Trental is shown from cardiovascular agents.
Fainting
Fainting (syncope)- an attack of short-term loss of consciousness, a kind of vegetative-vascular crisis, manifested by an acute violation of cerebral blood flow. These attacks occur in children with an unstable autonomic nervous system (ANS), cardiac pathology, more often in girls in the puberty period.
The etiology and pathogenesis of syncopal conditions (SS) have not yet been fully elucidated. It is impossible to exclude the role of "familial" latent viruses with their vertical transmission by the mother to children, which simulates the hereditary nature of the disease. The pathogenesis of SS is dominated by constitutional dysfunction of the hypothalamus and limbic-reticular complex in the form of a violation of the release of neurotransmitters involved in the regulation autonomic functions organism. However, dyscirculatory changes in the basins of the vertebral and carotid arteries, as well as a number of cardiogenic causes, may also be noted. In addition, in children with SS, delayed manifestations of perinatal encephalopathy (PEP) are found in the form of mild neurological signs of a residual organic nature, hypertensive-hydrocephalic syndrome, psycho-emotional, motor, endocrine and vegetative-visceral disorders. The inadequacy of the suprasegmental regulation of the ANS leads to the fact that such children remain vegetatively stigmatized for life and are extremely sensitive to external influences: mental trauma, painful stimuli, a sharp transition from a horizontal to a vertical position, overwork, intoxication. Occasionally, the causes of fainting can be a prolonged cough, the act of urination, defecation, sharp turns of the head. Vegetative disturbances become aggravated during puberty, after infectious and somatic diseases. However, the role of intercurrent infections in the pathology of the ANS is extremely moderate and always secondary.
There are numerous classifications of SS, due to the lack of a generally accepted concept of pathogenesis. Despite the conventionality, all variants of SS can be divided into neurogenic and somatogenic (usually cardiogenic). Among the neurogenic, there are vasomotor, orthostatic, vagal, hyperventilatory, cerebral, cough, hypoglycemic, nocturic, hysterical, associated with hypersensitivity of the carotid sinus, and mixed.
Clinical manifestations of all SS are stereotyped. In their development, three periods can be distinguished: the presyncope state, the syncope itself and the postsyncope period. The period of precursors is characterized by a feeling of discomfort, lightheadedness, dizziness, tinnitus, blurred vision, lack of air, the appearance of cold sweat, "coma in the throat", numbness of the tongue, lips, fingertips and lasts from 5 to 2 minutes. Loss of consciousness is observed from 5 s to 1 min and is accompanied by pallor, decreased muscle tone, dilated pupils, and their weak reaction to light. The breathing is superficial, the pulse is weak, labile, blood pressure is reduced. With deep syncope, tonic-clonic muscle twitches are possible, but pathological reflexes missing. After fainting, the child orients himself quite correctly in space and time, but may be frightened by what has happened, remains pale, adynamic, and complains of fatigue. He has rapid breathing, labile pulse, low blood pressure.
clinical picture. by the most frequent option SS is Vasodepressor syncope, In which there is a sharp decrease in peripheral resistance of muscle vessels and their dilatation, as well as a decrease in the volume of blood supplied to the heart, a decrease in blood pressure without a compensatory increase in heart rate (HR). In the pathogenesis of syncope, a violation of cerebral regulatory mechanisms plays a role cardiovascular systems s and the lack of inclusion of the "muscle" pump. Such SS often occurs during prolonged standing in a stuffy room, accompanied by many psycho-vegetative manifestations in the pre- and post-syncope periods. At orthostatic fainting, On the contrary, there is an instant loss of consciousness without paroxysmal manifestations when moving from a horizontal to a vertical position due to a drop in blood pressure with a normal heart rate. In children of this group, there is a delay in the release of catecholamines and an increase in the secretion of aldosterone in response to the orthostatic factor. For Vagal syncope Bradycardia, asystole, a sharp drop in blood pressure, loss of muscle tone, and respiratory failure are characteristic, since the fields in the reticular formation (net formation) that regulate these systems are close to each other.
Excessive breathing, hyperventilation, leads to alkalosis, a decrease in PCo2 in the blood, suppression of the dissociation of oxyhemoglobin, and polysystemic changes in the body in the form of a prolonged pre-syncope state, latent arrhythmias, paresthesia, and myofascial disorders such as carpopedal spasm. When you try to get up, repeated fainting is possible.
Patients with arterial hypertension often show hypersensitivity of the carotid sinus. With pressure on the carotid sinus, turning the head, while eating, vagal, vasodepressor or Cerebral Options SS. The latter option is based on a sharp deterioration in the blood supply to the brain with satisfactory hemodynamic parameters. There may be no presyncopal period, loss of consciousness is accompanied by a loss of muscle tone, a feeling of severe weakness due to increased sensitivity not only of the carotid node, but also of the boulevard centers. The post-attack period is characterized by asthenia, a feeling of unhappiness, and depression.
An attack of coughing can lead to a sharp increase in intra-thoracic and intra-abdominal pressure, swelling of the cervical veins, cyanosis of the face. With dysfunction of the central stem formations responsible for the regulation of respiration, vasodepressor and cardioinhibitory reactions are possible, as well as a drop in cardiac output as a result of stimulation of the vagus nerve receptor system. Similar mechanisms of SS are observed when the trigger zones of the glossopharyngeal and vagus nerves are irritated during chewing, swallowing, speech, urination and defecation.
Hypoglycemic syncope They are observed when the blood sugar concentration drops to 2 mmol / l or more (a reaction to hyperinsulinemia), brain hypoxia, as a result of which the child develops drowsiness and disorientation, gradually turning into a coma. Vegetative disorders are also characteristic: severe sweating, internal trembling, chill-like hyperkinesis (hyperadrenalinemia). When drinking sweet tea, all symptoms instantly disappear. Syncope of a hysterical nature Occur when conflict situation and the presence of spectators, are demonstrative in nature and are often a way of self-expression in neuropathic children. For kids early age(up to 3 years) are characteristic Fainting with cessation of breathing. They always begin with crying, then the child stops breathing, cyanosis appears. At the same time, the limbs are rigidly extended, convulsive movements are possible, after which relaxation and restoration of breathing occur. At an older age, these children have vasovagal SS. In young children, after head injuries, it is possible Pale type of syncope. At the same time, the child begins to cry, then turns pale sharply, stops breathing, he develops muscle hypotension. This state quickly normalizes. Such attacks are also associated with an increase in vagus nerve reflexes. The EEG is normal, which helps rule out epilepsy.
Cardiogenic syncope They arise as a result of a drop in cardiac output below the critical level necessary for effective blood flow in the vessels of the brain.
The most common causes of cardiogenic CV events are heart diseases leading to the formation of mechanical obstructions to blood flow (aortic stenosis, pulmonary hypertension with pulmonary artery stenosis, tetralogy of Fallot, atrial myxoma, cardiac tamponade) or rhythm disturbances.
Heart rhythm disturbances (primarily brady- or tachyarrhythmia) - common cause SS. In case of bradycardia, the child should be excluded from the syndrome of weakness of the sinus node, which occurs with organic damage to the atrial myocardium. Sinus node dysfunction is manifested by bradycardia less than 50 per minute and periods of missing ECG teeth - asystole. A classic example SS of arrhythmic origin is Morgagny syndrome-Adams-stokes, Characterized by the occurrence of attacks of sudden loss of consciousness, convulsions, pallor, followed by cyanosis, and respiratory disorders. During an attack, blood pressure is not determined and heart sounds are not heard. The periods of asystole can last for 5-10 s. Quite often such attacks are noted at transition of partial atrioventricular blockade to full. Less commonly, syncope occurs when the interval is lengthened. Q-T, Wolff-Parkinson-White syndrome, paroxysmal tachycardia, group extrasystoles. The following factors are of great diagnostic value: the presence of a cardiac history, a feeling of interruptions in the region of the heart before the onset of fainting, the connection of a sudden loss of consciousness without precursors with physical activity, ECG data. The prognosis for this variant of SS is worse than for neurogenic syncope. Cardiogenic SS is differentiated from various manifestations of epilepsy. At the same time, the role of the orthostatic factor, changes in hemodynamic parameters, and the absence of epilepsy-specific changes in the EEG are taken into account.
Emergency care and treatment for syncope:
And during an attack, you should give the child a horizontal position, loosen the tight collar, drink hot sweet tea and provide access to fresh air; And you can reflexively influence the respiratory and cardiovascular centers (inhalation of ammonia vapor or spraying the patient with cold water); And with a protracted course, injections of adrenaline or caffeine are indicated; And in the interictal period, it is necessary to carry out physical hardening, training for resistance to the orthostatic factor, and psychotherapy. The child should be taught the techniques of respiratory regulation, slowly getting out of bed. Useful gymnastics, skiing, running, various water procedures, exercise therapy, massage;
A course of restorative therapy, taking into account the predominance of one or another vegetative tone in a child. With vagotonia, askorutin, vitamins Wb and B|5, calcium preparations, tonics, nootropil, vegetotropic drugs (belloid, etc.) are used. In the case of sympathicotonia, vitamins B, B5, PP, potassium preparations, mild sedatives and beta-blockers (obzidan) are prescribed. Antiarrhythmic drugs are often used in cardiogenic syncope.
ACUTE LIVER FAILURE
Acute liver failure is characterized by the development of a severe general condition of the child with a sharp violation of all liver functions due to necrosis of its cells.
Etiology. Causes of acute liver failure: A liver disease (acute and chronic hepatitis, cirrhosis,
Neoplasms, alveolococcosis, etc.); A obstruction of the biliary tract and acute cholangitis; And diseases of other organs and systems (heart and blood vessels, connective tissue, infections); A hepatotropic poisoning toxic substances, poisonous
Mushrooms, drugs; And extreme effects on the body (trauma, surgery, burns, purulent-septic process, DIC, portal vein thrombosis).
clinical picture. Among the clinical symptoms, attention is drawn to icteric staining of the skin and mucous membranes, an increase in signs of hemorrhagic syndrome, a characteristic "liver" smell from the mouth, ascites, hepatosplenomegaly, neuropsychiatric disorders, the severity of which determines the degree of hepatic coma. At I degree, confusion, euphoria, sometimes depression, mental retardation, disorientation, tremor are noted; at II degree (precoma) - confusion, severe drowsiness, behavioral disorders; with III (stupor) - almost continuous sleep, sometimes agitation, severe confusion, disorientation, tremor; IV degree (coma) is characterized by loss of consciousness, lack of response to pain stimuli, muscle atony.
Intensive care: A restriction or cessation (in coma) of protein intake and
table salt; A parenteral nutrition - the introduction of 10% and 20% glucose solutions (120-150 ml / kg of body weight) with the addition of insulin (at the rate of 1 unit per 1 g of dry glucose); And intravenous administration of 10% solution of glutamic acid from 2 to 10 ml daily for 20 days and 10% solution of calcium chloride in age doses;
And high cleansing enemas, the appointment of laxatives (to reduce the absorption of protein and its decay products into the blood);
And the introduction through the tube of broad-spectrum antibiotics, metronidazole, enterosorbents, cimetidine, lactulose; the introduction of antioxidants, unithiol, antihypoxants, corticosteroids (intravenously, in high doses - from 7 to 20 mcg / kg / day per prednisolone), vitamins A, group B, C, K, riboxin, methionine, contrical, luminal;
A powerful hepatotropic effect is exerted by intravenous administration of 1 mg of glucagon in combination with 10 IU of insulin in 5% glucose solution, as well as large doses of L-dopa and solcoseryl with 5% glucose solution;
A hemo - and plasma transfusion, 20% albumin solution;
And hemosorption, plasmapheresis and hemodialysis - to remove toxins;
And the use of anabolic hormones (nerobol, retabolil) to improve metabolic processes in the liver.
ACUTE RENAL FAILURE
Acute renal failure (ARF) is characterized by impaired renal function with the development of azotemia, uremia, electrolyte, acid-base and volemic disorders.
OOP can be Prerenal(with a decrease in BCC, arterial hypertension, severe heart failure, liver failure), Renal(with acute tubular necrosis after prolonged ischemia or exposure to nephrotoxic substances, with damage to arterioles in cases of malignant arterial hypertension, vasculitis, microangiopathies; with glomerulonephritis, acute interstitial nephritis, metabolic disorders with intrarenal deposits) and Postrenal(with obstruction of the ureters and lower urinary tract).
The main objectives of therapy: A provision of forced diuresis for the purpose of dehydration,
Reducing uremic intoxication and hyperkalemia; A dehydration aimed at fast elimination extracellular fluid (introduction of diuretics, in particular lasix-sa - up to 12 mg / kg / day). With hyperhydration, accompanied by a sharp drop in potassium excretion and the development of hyperkalemia, it is advisable to cause artificial diarrhea with sorbitol (a 70% solution is administered orally at a dose of up to 250 ml); And to reduce the negative effect of excess potassium on the myocardium, intravenous administration of a 10% solution of calcium gluconate at a dose of 0.5 ml/kg in combination with hypertonic glucose solution is necessary.
Indications for hemodialysis:
▲ lack of positive dynamics with the introduction of large doses of diuretics (over 12 mg/kg of body weight);
▲ hyperkalemia (potassium content in blood serum over 6 mmol/l), metabolic acidosis (BE over 12 mmol/l), increased blood urea (21-25 mmol/l, its daily increase is more than 3-5 mmol/l) ;
▲ hyperhydration with an increase of more than 7% of body weight, pulmonary and cerebral edema.
In the fight against uremic intoxication and acidosis, conservative methods of extrahepatic blood purification are also used: siphon enemas (morning and evening) with the addition of 2% sodium bicarbonate solution, gastric lavage and skin toilet. In order to slow down the growth of azotemia, provide the body's basic need for calories and reduce catabolic processes in the body, patients are prescribed fractional meals (every 3-4 hours) with a sharp restriction of protein content in food. In arterial hypertension, often concomitant with acute renal failure, angiotensin-converting enzyme inhibitors are the drugs of choice. The most effective is the use of captopril in a daily dose of 1-8 mg/kg (administered with an interval of 6 hours). Calcium antagonists (nifedipine) can also be used.
BRAIN EDEMA
cerebral edema- a severe syndrome of non-specific CNS damage that develops with infectious and somatic diseases, acute neuroinfections, epistatus, cerebrovascular accident, skull trauma.
clinical picture. Main symptoms: headache, vomiting, impaired consciousness (from mild depression to deep coma) - indicate intracranial hypertension. One of the manifestations of cerebral edema may be convulsive syndrome.
Tasks of intensive care for cerebral edema:
▲ elimination of the underlying disease; And dehydration.
For the purpose of dehydration, intravenous hypertonic solutions are used (10% and 20% glucose solutions, 25% magnesium sulfate solution), colloidal solutions (reogluman, reopoliglyukin, reomac-rodex at the rate of 10 ml / kg / day), mannitol, mannitol (0.25 -0.5 g of dry matter per 1 kg of body weight per day), as well as diuretics (lasix - 1-4 mg / kg / day, aminophylline - from 6 to 8 mg / kg / day). To increase the osmotic pressure, albumin, plasma are administered, in order to improve microcirculation and brain metabolism - veno-ruton (6-8 mg / kg / day), cavinton (0.5-0.6 mg / kg / day), trental (3 - 4 mg / kg / day), nootropil (100-160 mg / kg / day), glutamic acid (10-12 mg / kg / day intravenously). The introduction of dexazone (0.2-0.4 mg / kg / day) and contrical (300-600 U / kg / day) is shown.
With convulsive syndrome - correction and maintenance
Vital body functions, conducting anticonvulsant
And dehydration measures. It is necessary to provide:
A free airway patency;
And oxygen therapy, with indications of mechanical ventilation;
A stabilization of hemodynamics;
And control over the state in single-electrolyte metabolism, acid-base balance (KOR), biochemical indicators of homeostasis. If any of these violations are present,
their immediate correction.
Anticonvulsant therapy:
And intramuscular or intravenous administration of a 2% solution of hexenal or 1% solution of sodium thiopental (2-5 ml) until the seizures stop. With the resumption of seizures, these drugs can be administered repeatedly. Seduxen, Relanium, 20% sodium oxybutyrate solution have a good anticonvulsant effect;
And for the purpose of dehydration, diuretics (lasix), a 25% solution of magnesium sulfate (at the rate of 1 ml per year of a child's life), and concentrated glucose solutions are administered.
CRAMPS
Seizures are sudden attacks of clonic or tonic-clonic involuntary muscle contractions with or without loss of consciousness.
There are general cramps and cramps of individual muscle groups. Their special variety are epileptic seizures.
Etiology. Seizures occur due to an organic or functional lesion nervous system. Convulsions of organic origin may be due to inflammatory, mechanical or vascular disorders, as well as the presence of a mass formation in the brain. Convulsions of functional origin occur with metabolic disorders (hypoglycemia, hypocalcemia, hypochloremia, etc.), transient vascular disorders, exposure to toxic or physical factors of a temporary nature. Allocate convulsions tonic, clonic, mixed - clonic-tonic, tetanic.
clinical picture. Regardless of the etiology, seizures are characterized by a sudden onset, motor excitement, impaired consciousness and loss of contact with the outside world. At the same time, the head is thrown back, the arms are bent at the elbow joints, the legs are extended, biting of the tongue, slowing of the pulse, slowing or short-term cessation of breathing are often noted. Such a tonic convulsion lasts no more than 1 minute and is replaced by a deep breath and the restoration of consciousness. Clonic convulsions begin with twitching of the muscles of the face with
Regression to the limbs. Then there are noisy breathing, foam on the lips, tongue bite, increased heart rate. Convulsions can be of varying duration and follow one after another; sometimes end in death. After an attack, the child falls asleep, and upon awakening, he may not remember anything and feel healthy. Tetanic convulsions are muscle contractions that follow each other without relaxation and are accompanied by pain. To determine the cause of convulsive seizures, it is necessary to collect a detailed history, conduct a thorough neurological and somatic examination, functional studies, blood, urine, and cerebrospinal fluid tests.
Seizures in children aged 1-6 months
The appearance of seizures in newborns and infants is due to their tendency to generalized reactions due to the high permeability of the blood-brain barrier and blood vessels, metabolic lability and sensitivity of the nervous tissue to various agents. Seizures may be caused by Anomalies in the development of the brain and skull. In this case, convulsions appear during the neonatal period, are more often tonic and are caused by defects in the brain (macro-, micro- and anencephaly) or skull bones (internal hyperostoses). To clarify the diagnosis, cranio- and pneumoencephalography is used, the karyotype (genetic damage) is determined.
convulsions Infectious (inflammatory) genesis Caused primarily by viral infections (rubella, herpes simplex, cytomegaloviruses - CMV). Brain damage in rubella is often combined with congenital heart defects, congenital cataracts, deafness, mental retardation, later with dental anomalies, etc. CMV brain damage develops simultaneously with jaundice, hepatic coma. CMV is determined in urine, saliva, puncture organ material. The herpes virus causes severe necrotizing encephalitis or meningoencephalitis, hepatitis with jaundice and hemorrhages. Bacterial infections are more often transmitted to the fetus not in utero, but intranatally (the cause of convulsions in this case is purulent meningitis or hyperthermia). Congenital toxoplasmosis Often accompanied by macrocephaly, microphthalmia, the formation of intracranial calcifications (often in the region of the subcortical nuclei), chorioretinitis pigmentosa, and atrophy of the optic nerves with loss of vision. If a congenital infection is suspected, bacteriological and virological studies should always be carried out simultaneously in the child and mother.
Seizures in newborns may be due to Immaturity, asphyxia Or Hemorrhages in the brain. In immature and premature babies, twitching of the limbs, rigidity,
eyeball conjugation; in full-term - unilateral convulsions, drowsiness. Hemorrhages in the fundus and blood-stained cerebrospinal fluid may indicate massive hemorrhage and hypoxic brain damage.
Tetanus In newborns and infants, it is characterized by a typical clinical picture - total tonic convulsions (opisthotonus) and trismus of masticatory muscles. It is currently very rare.
metabolic cramps Often due to a violation of the water-electrolyte balance during exicosis and rehydration. So, with inaccurately balanced infusion therapy (hyper - or hyponatremia), severe seizures with subsequent neurological disorders are possible. The causes of seizures can be hypoglycemia (with intrauterine dystrophy of the fetus or in a child whose mother has diabetes), hypocalcemia (with rickets, hypoparathyroidism and pseudohypoparathyroidism), hypomagnesemia (congenital, with poor or poor nutrition, malabsorption syndrome). For differential diagnosis, biochemical analyzes of blood and urine are carried out, the content of hormones in plasma is determined. The absence of acute-phase indicators of inflammation confirms the possible metabolic nature of the disorders.
Iatrogenic convulsions Associated with taking high doses of drugs and / or with poor (slow) release from the body (caffeine, penicillin, etc.).
Violation of amino acid metabolism(phenylketonuria, histidinemia, maple syrup disease, homocystinuria, tyrosinosis, etc.) is diagnosed by chromatographic examination of urine and serum. At the same time, there is often a delay in mental and motor development and convulsions.
Seizures in children older than 6 months
In children of this age, the development of non-epileptic seizures should first be excluded.
Febrile convulsions(under the age of 3 years) often occur before an increase in body temperature or at the height of a febrile reaction. They, as a rule, do not occur in children under 6 months and older than 4 years. Frequent seizures (more than 3 times a day), focal or predominantly unilateral seizures, subsequent development of paresis and the presence of pathology on the EEG indicate the impossibility of the occurrence of febrile seizures. In this case, a lumbar puncture should be done to rule out meningitis and encephalitis.
Hemorrhage in the brain Or vascular disturbances may cause sudden unilateral and then generalized convulsions with fever, impaired consciousness and subsequent paralysis. Their immediate causes may be aneurysm
Rhysms, embolism of the middle cerebral arteries or their branches, venous thrombosis, abscesses, thrombocytopenic purpura, systemic lupus erythematosus (SLE), systemic vasculitis, sometimes fibromuscular hyperplasia of the cerebral arteries, diagnosed with repeated angiography. Eclamptic or pseudo-uremic convulsions Can be The initial symptom of acute nephritis(In the diagnosis, an increase in blood pressure is important).
Syncope- short-term loss of consciousness with short generalized tonic-clonic convulsions (vasal reflex reactions with vasomotor collapse) are not uncommon in children older than 4 years and especially in puberty. To establish the diagnosis, it is important to measure blood pressure (low), to identify arrhythmia or paroxysmal tachycardia, and the presence of a previous stressful situation.
brain tumors They can provoke both focal and generalized seizures, most often when they are localized in the posterior cranial fossa of the brain. Tumors grow slowly, and short-term convulsions may be the only symptom of the disease for a long time. In these cases, it is very important to conduct a diagnostic search: EEG, angiography, scintigraphy, computed and magnetic resonance imaging. Seizures may be caused by a brain pseudotumor. This is a peculiar condition caused by restriction of venous blood flow in otitis media with sinus thrombosis, limited encephalitis or adhesive arachnoiditis. The diagnosis can be confirmed by a thorough examination of the patient and dynamic observation of him.
Rarer causes of seizures include tuberous sclerosis(pseudotumor nodular growths in the brain with the accumulation of glycogen). Convulsions in this pathology are generalized, clonic-tonic. The child lags behind in mental development. The diagnosis is confirmed by the presence of intracranial areas of calcification, tumor-like formations in the retina and brownish papular rashes on the skin of the face.
brain abscesses Sometimes they are manifested by convulsions without inflammatory laboratory signs (decrease in ESR, slight leukocytosis) and increased intracranial pressure.
Getting into the brain With blood flow Ascaris larvae, Finn porcine Or dog tapeworm Causes convulsions, often in combination with impaired craniocerebral innervation, ataxia, aphasia, meningism, hydrocephalus, psychotic behavior. Identification of calcified areas in the brain, protein and eosinophilia in the cerebrospinal fluid, eosinophilia in the blood and antibodies in the serum makes it possible to clarify the diagnosis of helminthiasis.
Convulsions of infectious (bacterial) origin In children of any age, most often due to coccal flora. Meningo-coccal meningitis is manifested not only by convulsions, but also by fever, vomiting, hyperesthesia, tension of the large fontanelle or its bulging (in children of the first year of life) and typical
Morragic stellate rash. In other coccal infections, meningitis is combined with tonsillitis, pneumonia, otitis media, peritonitis, etc. In differential diagnosis, it is important to take into account changes in the cerebrospinal fluid (the number and type of cells, the concentration of protein, sugar, chlorides, the presence and type of microbe). Candidiasis meningitis is very rare and is usually diagnosed in cases of generalized candidiasis.
The causes of seizures in both younger and older children can be Copper metabolism disorders And Decrease in the content of ceruloplasmin in blood plasma(diseases of Konovalov-Wilson and Menke). In Konovalov-Wilson disease, hyperpigmentation of the cornea (Kaiser-Fleischner rings) is observed in combination with liver pathology; in Menke disease, hypothermia, brittleness and thinning of hair, dementia, rickets-like bone changes, lengthening and tortuosity of arteries (with angiography).
In etiologically unclear cases of seizures in combination with delayed psychomotor development, the presence of metabolic disorders in patients should always be excluded, primarily amino acid metabolism disorders, then protein, fat and carbohydrate metabolism.
psychogenic seizures They are divided into respiratory, hysterical and hyperventilatory. Respiratory spasms are observed in children 1-4 years of age after a mild injury or infection. At the same time, the child cries out, he has a respiratory pause, accompanied by cyanosis, twitching (until breathing is restored). In other cases, the child continuously screams without inhaling, to the point of deep cyanosis ("rolls over"). Muscular hypertonicity appears up to opisthotonus and clonic-tonic convulsions. Their reason is hypoxia on the background of affect. EEG is practically unchanged, especially outside the attack.
hysterical seizures They occur in school-age children and usually imitate seizures. The frequency of twitches is less than with true clonic seizures, and tonic seizures are worm-like in nature. In addition, there are no typical signs of autonomic disorders (sweaty, pale face, salivation, involuntary urination at the end of a seizure, biting of the tongue, etc.). EEG - no changes.
Hyperventilation tetany It is more often noted in children in the puberty period, caused by an effort of will or fear, combined with palpitations, paresthesias, respiratory alkalosis. The attack is removed when breathing into a plastic bag without air access. Sometimes hyperventilation convulsions are observed in stem encephalitis.
epileptic convulsions They are observed at different ages: infancy, preschool, school, puberty and differ in clinical manifestations and typical EEG changes. There are idiopathic (genuine, unknown etiology) and residual (due to brain damage in early childhood,
Nuclear jaundice, trauma, hemorrhage, congenital anomalies, inflammation) epilepsy. In most cases, confirmation of the diagnosis is possible with dynamic clinical observation and repeated EEG studies.
epileptic seizures
There are propulsive small, large and focal epileptic seizures.
Propulsive minor seizures Develop in infants. They are characterized by repeated flexion movements of the torso and head with throwing up the arms and bending the legs. Lightning convulsions (lasting a few seconds) with loss of consciousness are possible, recurring throughout the day, especially after waking up. In these cases, the EEG shows mixed diffuse convulsive activity. AT before school age observed Myoclonic jerks With an acute loss of muscle tone, rapid falls, bouts of nodding, blinking and screaming, as well as "absences" - shutdowns. Their duration is 1-2 s. At the same time, there are often twilight states, later - a delay in psychomotor development. On the EEG - generalized bilateral synchronous irregular peaks, as well as sharp and slow waves.
At school age, the manifestations of small seizures are different: loss of consciousness, half-open eyes, swallowing, licking, chewing or pulling movements, rhythmic twitching of the muscles of the face, hands for 5-30 seconds - most often in the morning or when tired; EEG shows generalized bursts of bilateral peaks and waves.
At puberty, there are symmetrical myoclonic seizures with tossing of hands without loss of consciousness, more often upon awakening, lack of sleep. They are isolated or in the form of volleys and last for several seconds or minutes.
Grand mal seizures of epilepsy Possible at any age. In 10% of cases, a grand mal seizure is preceded by an aura (a period of precursors). Then the child falls screaming, he has a tonic convulsion lasting up to 30 seconds with opisthotonus, apnea, cyanosis and transition to clonic convulsions lasting up to 2 minutes, with salivation, sometimes vomiting, involuntary urination, defecation and subsequent falling asleep. Seizures may occur during sleep or before awakening, sometimes associated with psychomotor or focal seizures. On the EEG - general changes and peaked waves at rest (provocation by hyperventilation or insomnia).
Focal seizures (Jackson epilepsy) Characterized by aura, localized clonic twitches, sometimes transient partial paresis; lasting seconds, minutes or hours. On EEG-focal or multifocal foci of convulsive activity with sleep provocation. In most cases, Jacksonian epilepsy is the result of an injury, inflammation, or cerebral hemorrhage that was previously transferred, often in the neonatal period.
Shock
Shock- a syndrome characterized by severe disorders of the central and peripheral circulation, respiration, metabolism, all types of metabolism, depression of the central nervous system.
In pediatric practice, the following types of shock are most often observed:
▲ hemorrhagic or hypovolemic - with massive blood loss or severe dehydration of the body;
▲ traumatic - with severe trauma, surgical interventions, lesions electric shock, burns, sudden cooling, compression of the body;
▲ toxic-septic - in severe infectious and septic processes;
▲ anaphylactic - as a result of allergic reactions when administered medicines, vaccines, serums, transfusion of protein preparations, etc.
clinical picture. There are 3 phases of shock: erectile, torpid and terminal. In the first phase, due to an excessive flow of impulses from the pathological focus, generalized excitation of the nervous system occurs. Clinically, this is manifested by an increase in motor activity, shortness of breath, tachycardia, and an increase in blood pressure. The second phase of shock is characterized by deep inhibition of the nervous system due to its overexcitation in the first phase. A disorder of nervous regulation causes severe disturbances in blood circulation, respiration, and the functions of the endocrine system, primarily the adrenal glands. The immediate cause of the threat to the life of the patient in shock are violations of hemodynamics and gas exchange. In the torpid phase, hypotension rapidly increases and BCC decreases (by 25–40% in hemorrhagic or hypovolemic shock), and centralization of blood circulation occurs, caused by spasm of the capillary network. With the further development of the state of shock, gas exchange disorders are aggravated due to changes in the bcc, microcirculation disorders, respiratory center depression, hypofunction of the adrenal glands. As a result of these disorders, renal blood flow decreases, up to acute renal failure. Shock is necessarily accompanied by DIC, and often by convulsions (due to cerebral edema).
Treatment. The goal is to maintain hemodynamics with the help of intravenous fluid infusions, vasopressors, agents with a positive inotropic effect (dopamine, dobutrex), corticosteroids. Intensive therapy begins with a rapid replenishment of the BCC by the introduction of saline, colloidal solutions and blood products. If necessary, an emergency correction of blood clotting disorders and electrolyte balance is carried out. The use of adrenaline, dopamine is shown. In the absence of a risk of bleeding, heparin (100-300 U/kg/day) should be used, as well as inhibitors of the kallikrein-kinin system (gordox, contrical, trasilol). For detoxification and improvement of microcirculation, low molecular weight dextrans are used (rheopolyglucin, hemodez). In traumatic shock, the trigger mechanism for microcirculation disorders is the flow of pain impulses. Analgesia and blockade of pain impulses prevent spasm in the microcirculation system. Infusion therapy, taking into account the replenishment of the BCC deficiency and the improvement of the rheological properties of the blood, is similar to that carried out with hemorrhagic shock.
burn shock It develops as a result of superstrong pain irritation emanating from an extensive wound surface, and toxemia. feature clinical picture burn shock is a more pronounced and prolonged erectile phase. In this case, the torpid phase is characterized by acute renal failure. General principles therapy is almost the same as described above. Special attention should be given to the treatment of renal failure.
Toxic-septic shock It is characterized by the development of acute cardiovascular failure due to intoxication caused by a septic process. It is clinically manifested by a sudden deterioration in the condition, first by hyper- and then by hypothermia, a drop in blood pressure, and severe microcirculation disorders. Consciousness is confused, up to the development of coma. Growing signs of acute renal failure (ARF). The peculiarities of therapy include intravenous administration of broad-spectrum antibiotics, the use of hyperimmune drugs, and large doses of corticosteroids.
Anaphylactic shock It is a severe allergic reaction, proceeding according to the type of acute cardiovascular and adrenal insufficiency. The basic principles of treatment are similar to those outlined above, but in this case, multiple administration of corticosteroid hormones, antihistamines, adrenaline and its derivatives, and heparin should be added. With edematous syndrome, dehydration therapy is carried out.
| ← ENKOPRES | VARIANTS OF JAUNDICE IN CHILDREN → |
|---|
Chapter 10
Allergic shock (anaphylactic shock)
Children respond to various intolerable factors to a much greater extent than adults. If a child comes into contact with such harmful substances, then an allergic reaction occurs. It could be bee or wasp venom. food products(most often cow's milk, chicken protein, fish, nuts), medicines or allergens that enter the body through breathing (pollen, animal hair). With high sensitivity to these allergens, both local manifestations are possible, as we have already discussed, and general reactions body - up to shock with impaired functions of the respiratory and cardiovascular systems. This process is not associated with mental shock that occurs with significant emotional stress.
The clinical picture of shock is usually beyond doubt. The skin of the child is pale, cold sweat appears. The pulse is frequent, difficult to determine. Breathing is frequent, shallow. Consciousness is confused, further loss of consciousness is possible. In allergic shock, respiratory failure (suffocation) associated with swelling of the mucous membrane of the respiratory tract, as well as swelling of the face and skin manifestations, is possible.
At the slightest suspicion of shock call a doctor immediately!
Experience shows that most parents who are aware of the predisposition of their children to allergic reactions have at home, in agreement with the attending physician, the appropriate emergency medicines to be used.
Until the ambulance came
In many cases, a wonderful effect can be obtained from homeopathic medicines.
Apis mellifica D200, 1000 take 2 grains of any one at hand; if necessary, you can repeat the reception. The drug is effective for allergic blisters and urticaria (nettle fever) of any severity, as well as for swelling of the conjunctiva, eyelids, lips, mouth.
Acidum carbolicum D200 is given to the child once - 2 grains. It is an adjunct in anaphylactic shock with dysfunction of the cardiovascular and respiratory systems.
false croup
This is one of the special forms of laryngitis (inflammation of the larynx). The mucous membrane below the level of the vocal cords is inflamed and edematous, which greatly complicates the passage of air when the child breathes. Since the name "croup" was associated with diphtheria in earlier times, this disease, which has similar symptoms, is designated as "false croup". The disease is usually associated with viral infection, so it is most common in the cold season.
Sometimes, often unexpectedly and at night, suddenly there is a dry barking, rough cough and wheezing on inspiration - signs of suffocation. This is the so-called false croup. Such a lack of breathing is expressed primarily in anxiety and fear, and can even lead to loss of consciousness. In children under one year old, this disease is rare, because, apparently, maternal immunity plays a large role. Most often, false croup occurs in the second year of life, and boys are more susceptible to this pathology than girls. As the child grows, the possibility of the disease becomes less and less. If you know that your child has a tendency to it, spend more in the fall, from the beginning of September, preventive treatment. As one old pediatrician noted, foggy autumn provokes attacks of coughing.
Experience has long been accumulated in the treatment of this process by natural means.
First aid for an acute attack
The most important thing for parents is to remain calm, not to lose their head and try to calm the child, because the more he is afraid, the worse he feels.
At the same time, you need to take care of a sufficient supply of fresh and cool air.
Try increasing the humidity in the room: put on hot battery wet towel, turn on in the bathroom hot water(steam should not be scalding); in case of repeated diseases, it is better to purchase a special humidifier for a battery or apparatus.
It is advisable to make a warm foot or general bath with a water temperature of 37–40 ° C, and mustard can be added to the foot bath (2 tablespoons per bucket of water). Mustard plasters can be placed on the chest, wrapping the child well.
Sometimes warm compresses on the neck and warm drinks help: milk with soda or Borjomi, fruit drinks, etc.
Physicians practicing anthroposophic methods actively use the simplest and effective remedy. Needs to be cut into small pieces onion, mix with a little oil, heat this mass in a pan for so long until the onion becomes transparent (but do not fry!). Put everything on a cloth, cool to a warm state, cover it with a thin cloth on top and put it on the larynx, and wrap it with a woolen scarf on top. Usually after 2-3 minutes the attack passes. The same compress can be done prophylactically if you know that your child has already had attacks of false croup, you notice that the child has a cold, and you have a suspicion that your child may have an attack at night. In this case, it is better to make a compress for the night.
Homeopathic preparations
In an acute attack of coughing, give 5 grains every 5 minutes in turn the following drugs - Spongia D6, Rumex D6, Sambucus D6, Apis D6.
When improvement occurs, the intervals between taking medications are lengthened (10–20 minutes). You can put a hot infusion of chamomile nearby for evaporation. Experience shows that in most cases, such treatment can prevent the prescription of hormones (corticosteroids). In extreme situations, however, cortisone suppositories should not be abandoned. If the symptoms are dramatic, you need to consult a doctor.
Anthroposophic preparations
Bryonia/Spongia comp. relieves an attack well if you give a remedy for 3-5 grains every 10 minutes.
Larings D30 is an organ preparation of the larynx that allows you to relieve an attack instantly, so if your child is prone to such attacks, we recommend that you always have this drug ready in the cold season.
Autumn prevention of false croup
It is advisable to take 3 drugs: Spongia D12, Rumex D12, Aconite D12 - 5 grains of each remedy 1 time per day (in the morning - Spongia, in the afternoon - Rumex and in the evening - Aconite), a course of at least a month.
convulsions
Seizures are a fairly common condition in children. There are many reasons for their occurrence: an increase in body temperature above 39.5 ° c, infection, acute poisoning, brain damage. With convulsions in the muscles and limbs, twitches may occur, and in some cases, on the contrary, tension of the limbs develops with their maximum extension. During convulsions, the child seems to freeze with his head thrown back and his arms and legs convulsively stretched forward. This state can last from a few seconds to 10 minutes or even longer. In some cases, convulsive twitches are noted only in certain muscle groups and may go unnoticed by parents. During an attack of convulsions, the child, as a rule, loses consciousness, the eyes close, twitching is possible in the eyelids and other facial muscles, and the teeth are tightly clenched. Sometimes foam appears on the lips. Often there is involuntary urination. During an attack of general convulsions that lasts more than 2 to 3 minutes, the child's lips may suddenly become bluish as breathing becomes temporarily interrupted and spasmodic.
Parents should know that any sudden loss of consciousness with convulsions for the first time requires immediate medical advice.
First aid before the doctor arrives
If your child suddenly has seizures, try not to panic (although the sight of a child with seizures is really scary), your composure in this moment the child really needs. Take simple steps to ensure that your child is not hurt during an attack.
First of all, without moving the child, turn him on his side so that he does not choke on saliva.
Make sure that there are no hard and sharp objects near his head that he could get hurt during an attack.
After making sure that nothing is obstructing the baby's breathing, place a hard but not sharp object between the baby's teeth so that he does not accidentally bite his tongue - this can be anything that is at hand, for example, a folded leather glove (but not a finger!) or wallet.
After these events, you can call the doctor.
After an attack, it is necessary to transfer the child to the bed, free from disturbing clothing and allow him to sleep.
After an attack, the child is drowsy, therefore, for 1–1.5 hours, food and drink should not be given to him so that he cannot choke due to drowsiness.
If the child has a high temperature, before the doctor arrives, you can begin to reduce it as indicated in the section on temperature.
If you stay in a stuffy room for a long time or stand in one place for a long time (during ceremonial events, etc.), the child may faint. In rare cases, this can happen when you suddenly change your position, such as getting out of bed quickly. Sometimes the cause of fainting can be nervous tension such as when taking a blood test.
Fainting occurs due to insufficient blood circulation to the brain, as a result of which the child loses consciousness and falls. Before that, he experiences discomfort, turns pale, the skin is covered with cold sweat, there is tinnitus and nausea. Most often, having fallen during a faint, the child quickly comes to his senses, since in a horizontal position the blood enters the brain more intensively.
First aid
If a child who has lost consciousness has time to be supported, he should still be laid down. Raise your legs, lower your head to facilitate blood flow to the head. The room needs a window to open to allow access fresh air. It is necessary to free the child from tight clothing, unbutton the buttons on the neck, loosen the belt or strap. You can splash your face with cold water, rub your whiskey with a cotton swab dipped in ammonia, and let it smell.
In the hall, in a narrow passage between rows of chairs, they leave the unconscious person in place, in a sitting position, tilt the torso forward so that the head hangs as low as possible (due to compression of the abdomen, the blood flow rushes to the heart and head). The child should be allowed to stay in this position until recovery of good health, but not less than 5 minutes.
Homeopathic preparations
Aconite D30 is given once 5 grains when fainting from fright.
Ipecac D6 is shown in 3 grains every 10-15 minutes if fainting is associated with disgust at the sight of blood.
Ipecac D6 or Carbo vegetabilis D6 is recommended in the above doses for significant heat or stuffiness.
Nux vomica D6 has a positive effect after mental fatigue, it is given in 3-5 grains after 2 hours.
Solar and heat stroke
This condition is associated with overexposure sun rays on your child's uncovered head and neck. Prolonged exposure without protection high temperature or in the sun, especially when physical activity, leads to overheating of the head and brain and ends with sunstroke.
You should always think about the fact that on hot days the child drinks a lot (juices, water or a mixture thereof). Make sure that the child, especially on vacation in warm countries, does not fall asleep in the sun. In extreme heat, especially with pronounced humidity, you should be in the shade more. In summer, do not leave your child alone in a closed car, as the temperature often rises sharply in it.
Symptoms sunstroke manifest very energetically: the head becomes hot, the face turns red, headaches, anxiety, dizziness, nausea to vomiting, a state of stunned, in the worst case, an unconscious state appear. If at the same time the body temperature rises sharply to 40 ° C, then they speak of heat stroke. The condition worsens, loss of consciousness and convulsions are possible.
First aid
In case of sunstroke, especially in severe cases of heat stroke, there is a need for urgent medical care. Before the arrival of the doctor, it is necessary to lay the child in the shade, slightly raising his head, for example, laying the person accompanied by him on his knees. Wet a cotton handkerchief with cold water, wring it out and put it on the head and forehead, the body should be wiped with a towel soaked in cold water. Repeat the procedure after 10 minutes.
Homeopathic preparations
Camphor D3 - as the first remedy, the drug should be given in 3-4 doses of 3 grains every 10 minutes, and then Cactus D3 in 2 doses after 10 minutes, and then repeated after 1-2 hours. You can give Camphor and Cactus at the same time using the “glass of water method”.
Aconite D3 and Belladonna D3 or Gelsemium D3 and Glonoin D3 are also very effective when used with their "glass of water method".
Apis D6 is indicated for severe headache and tension in the occipital region - 5 grains 3-4 times a day.
Natrium carbonicum D12-30 is useful when, after suffering a sunstroke, complaints of temperature, headaches, dizziness, inability to think when exposed to the sun reappear; accepted in the same way.
In case of an unstable state of blood circulation or loss of consciousness, call a doctor immediately.
poisoning
If a poisonous substance enters the body, it leads to poisoning, causing disturbances in life, and sometimes death. The most common causes of poisoning are medicines, household chemicals (acetic acid, turpentine, soapstone solution, gasoline, household insecticides), poisonous plants and berries (wrestler, dope, henbane, wolfberries, hemlock, wild rosemary, marsh bogulnik, etc.), poisonous mushrooms, means for the destruction of agricultural pests (herbicides), fertilizers, washing powders and other detergents, gas.
Most of the poisoning occurs in early childhood and preschool age, when, due to extreme curiosity, children, without hesitation, take all sorts of objects into their mouths. Beautiful packaging liquids may lead them to think it's delicious lemonade. Naturally, poisoning can often be prevented, but, unfortunately, some parents realize this when the misfortune has already happened.
Medicines and remedies household chemicals must be out of reach of children!
The initial symptoms of poisoning may be severe nausea, vomiting, and abdominal pain. In case of poisoning chemicals the child may become lethargic, drowsy, indifferent, and in some cases the reverse picture is possible - extremely excited. Perhaps a balance disorder, convulsions, loss of consciousness.
Sometimes the child feels relatively well at first, but deterioration may develop gradually if the toxic substance is absorbed slowly in the stomach. Even 1-2 tablets of sleeping pills, antipyretics or heart medications can cause severe, sometimes fatal poisoning.
First aid
In all cases, a doctor should be consulted, even if the origin of the poisoning is known. If you find that the child ate (or drank) some drugs or chemicals, you must definitely take the package (vial) to the hospital so that the doctors can pick up the necessary antidote.
The task of first aid in case of poisoning food is the fastest removal of poison from the body. To do this, immediately do a gastric lavage. Give your child plenty to drink warm water, then take him in your arms and bend over a basin or bucket and induce vomiting by pressing a finger or a spoon on the root of the tongue. When washing again, you can add a 1% solution of baking soda to the water (1 teaspoon of soda per 0.5 l of water).
In case of poisoning with corrosive substances (alkalis, acids) cannot be induced to vomit because way back these fluids secondarily damage the esophagus. In this case, immediately give a plentiful drink (water, tea) to liquefy the toxic substance in the stomach.
Whatever the cause of poisoning - Chemical substance, plant, medicine or gas - the main task of parents is immediate call for an ambulance, because any ongoing activities before the arrival of the ambulance may be ineffective. And here the most logical and most expedient solution is hospitalization.
After eating poor-quality food, effective remedies are recommended.
Homeopathic preparations
Nux vomica D6 is great for stomach fullness, bloating, nausea, vomiting, and constipation.
Veratrum album D6 is useful in vomiting and diarrhea associated with the intake of poor-quality products.
Chamomilla D6 relieves vomiting with abdominal pain.
Sepia D3 and Okoubaka D6 are effective in poisoning with poor-quality fish.
Pulsatilla D3 is given for poisoning due to the use of fatty foods, pies, pastries.
All of these drugs can be given using the "glass of water" method.
Burns of the esophagus
This is a lesion of the mucous membrane of an organ, resulting from an accidentally drunk strong acid or alkali. This usually happens with curious young children attracted by unknown bottles. They may contain concentrated vinegar or hydrochloric acid, ammonia or a solution of potassium permanganate (potassium permanganate). The severity of the burn of the oral cavity, pharynx and esophagus depends on the amount of liquid swallowed. Since the burn causes severe pain, the child begins to scream loudly.
First aid
First of all, you need to quickly find out what the child swallowed. Before the arrival of the ambulance, the face and mouth of the child should be washed abundantly for several minutes with cold water. running water. You need to make sure that water does not flow into the eyes. The child's mouth can be rinsed with a rubber bulb. To dilute the acid or alkali in the esophagus and stomach, give the child a glass to drink. cold water or milk, but not more than the indicated dose, so as not to induce vomiting. Often, due to the prevalence of the process, the child has to be hospitalized in the hospital.
I would like to remind parents about the rules for storing strong and toxic substances. After all, misfortune can happen to an adult, if you do not put things in order.
From the book Anesthesiology and Resuscitation: Lecture Notes authorLecture No. 5
From the book Anesthesiology and Resuscitation: Lecture Notes author Marina Alexandrovna KolesnikovaLecture No. 6. Emergency conditions in cardiology 1. Myocardial infarction Myocardial infarction is a discrepancy between myocardial oxygen demand and its delivery, resulting in limited necrosis of the heart muscle. The most common cause is a thrombus, less often -
author Arkady Lvovich Vertkin From book Ambulance. A guide for paramedics and nurses author Arkady Lvovich Vertkin From the book Ambulance. A guide for paramedics and nurses author Arkady Lvovich Vertkin From the book Ambulance. A guide for paramedics and nurses author Arkady Lvovich Vertkin From the book Ambulance. A guide for paramedics and nurses author Arkady Lvovich Vertkin From the book Nursing: a guide author Alla Konstantinovna MyshkinaChapter 4 Emergencies Management of emergenciesAnaphylactic shockAnaphylactic shock develops in response to the introduction of a foreign protein. All therapeutic measures are carried out immediately, comprehensively. To do this, you should: 1) lay
author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From the book Emergency Handbook author Elena Yurievna Khramova From book Complete reference symptoms. Self-diagnosis of diseases author Tamara RutskayaThe doctor providing emergency care at the prehospital stage, according to the age of the child and the corresponding age-related anatomical and physiological features, should determine the specifics of the emergency condition in the child.
Anamnesis is the most important component of emergency diagnostics at the prehospital stage. In contrast to adults, in young children, the diagnosis is made in almost 50% of cases according to the anamnesis and only in 30% - according to the results of a physical examination.
Emergency conditions in children
What should doctors consider when diagnosing emergency conditions in children?
- Lack of constant monitoring of the patient.
- The possibility of developing a critical condition in children of the first year of life in the first minutes or hours after visiting a doctor against the background of a previously relatively satisfactory condition upon examination.
- Anatomical and physiological differences in the child's body.
- Often low sanitary and household culture of the population.
This explains the priority of tactical overdiagnosis (“weighting” of syndromes) during hospitalization of most patients during the first months of life.
The primary task of examining a child is to identify syndromes that determine the patient's condition, and not the cause of the disease. When making a diagnosis, the media doctor, unlike doctors in most other specialties, must go from the effect to the cause.
How are emergency conditions diagnosed in children?
- initially, the degree of violation of vital functions and the need for emergency therapeutic measures for health reasons are assessed;
- then the state of the central nervous system (the level of consciousness, the presence of cerebral symptoms, convulsive syndrome), central hemodynamics, respiration is determined and, if necessary, urgent measures are taken.
The study of the functions of vital organs and systems, as well as the correction of their disorders in children and adults, do not have fundamental differences.
If the state of the central nervous system, central hemodynamics and respiration are sufficiently stable, then the doctor proceeds to a typical examination of the patient.
Given the limited time, the EMS doctor collects only the data necessary to develop the required tactical decision and the volume of urgent measures.
History of children in the diagnosis of emergency conditions
- change in child's behavior
- hypodynamia, lethargy or hyperactivity,
- change in appetite
- sleep disturbance,
- drowsiness and lethargy in a normally active child - this may be a symptom of CNS depression,
- regurgitation, vomiting, one-two liquid stools in young children do not necessarily indicate an infectious lesion of the gastrointestinal tract, this can be the beginning of any disease,
- the presence of a previous perinatal pathology of the nervous system and its consequences to exclude the possibility of its manifestation,
- How did pregnancy and childbirth go?
- Is the child being seen by specialists?
- clarify the possibility of developing the disease against the background of intrauterine infection, malnutrition, rickets, perinatal pathology, congenital malformations, etc.,
- information about vaccinations, post-vaccination reactions,
- contacts with infectious patients,
- allergic history.
Physical examination of children in an emergency is aimed at identifying threatening conditions.
The complexity of examining young children is due to the peculiarities of their anatomical, physiological, psychomotor and speech development. So, newborns experience a number of borderline conditions (physiological weight loss, jaundice, dyspepsia, etc.), have physiological tachycardia (120-140 per 1 min) and tachypnea (40-60 per 1 min), etc.
In children, it is necessary first of all to identify decompensation of respiration, blood circulation and the degree of damage to the central nervous system.
Respiratory failure in an emergency
- absence,
- bradypnoe,
- pathological type.
Circulatory disorders in the diagnosis of the patient's condition
- the disappearance of the pulse on the radial artery with blood pressure below 50-60 mm Hg. Art.,
- the disappearance of the pulse on the carotid artery with blood pressure below 30 mm Hg. Art.,
- tachycardia,
- bradycardia,
- arrhythmia,
- "marbling" of the skin,
- cyanosis.
Children's Emergencies - CNS Research
- the level of consciousness when verbal contact is impossible is determined by the activity of the child, by the way he watches you and objects, whether he plays with a toy, how he screams or cries (a monotonous cry is characteristic of meningitis),
- diffuse cerebral reactions,
- convulsive syndrome (febrile convulsions),
- nonspecific toxic encephalopathy (neurotoxicosis),
- pupil width, their reaction to light,
- muscle tone, etc.
If meningitis is suspected, the doctor should remember that in children under 3 months of age, Kernig's symptom is physiological, and Brudzinsky's symptoms are rarely detected, but stiff neck, hyperesthesia to all stimuli, elements of the "pointing dog" position, monotonous cry and easy detectable symptom of "suspension".
Helping children with emergencies
The sequence of actions of an ambulance doctor at the prehospital stage
Child examination:
- Establish contact with parents to collect anamnesis and ensure the calm state of the patient during the examination.
- Get answers to questions:
- the reason for petition;
- circumstances of illness or injury;
- the duration of the disease;
- time of deterioration of the child's condition;
- means and preparations used before the arrival of the ambulance doctor.
Making a tactical decision(taking into account the fact that decompensation of the condition in children occurs faster than in adults!):
If a:
- the disease does not threaten the life of the patient;
- the state is stable;
- the material and living conditions of the child's life are satisfactory and he is guaranteed necessary care, excluding a threat to his life - you can leave the child at home with the mandatory transfer of an active call to the clinic.
If a:
- the nature and severity of the disease threaten the life of the patient;
- poor prognosis of the disease;
- unsatisfactory social environment and the age of the child suggest treatment only in a hospital - hospitalization of the child is necessary.
If the parents refuse to be hospitalized, it is necessary to report this to the senior doctor of the EMS station and act on his instructions. Any refusal of examination, medical care, hospitalization must be recorded in the EMS doctor's call card and signed by the child's parent or guardian. If the patient or the parent (or guardian) of the child does not want to issue a waiver of hospitalization in statutory form, it is necessary to involve at least two witnesses and record the refusal. Now you know how children are cared for in emergencies.
Read also...
- Education of the USSR: prerequisites, stages, significance When the USSR was created
- Education of the USSR: briefly about everything What led to the formation of the USSR
- Socialist-Revolutionary Party: who are they? Their goals and program. Political parties at the beginning of the 20th century Socialist-Revolutionaries party program table briefly
- Vitaprost rectal suppositories: how to use the drug correctly You can take Vitaprost without a doctor's prescription

















